Source: www.indiangyan.com/books/therapybooks/ Osteopathy/Headaches_Migraine.shtml A headache is a common problem today. Who does not get a headache? An executive, a philosopher, a scientist, a business magnate, a clerk, a housewife, a student - everybody, at sometime or other, is afflicted by a headache! It has no professional or age barriers.
Women suffer more than men. The reason may well be pre-menstrual migraines during puberty. These get worse as the years roll by, and are cured only by menopause. Contraceptives are known to cause headaches in some women and cure them in others. Headaches may become less frequent in pregnancy. In fact, a headache is not a killing disease, but its attack is so intense that all the nerves in the skull start throbbing due to great pressure.
A lot of research has been done to find out the cause of headaches.
What is a headache? Is it an allergic disease caused by something we eat or breathe? Has it any relation to our posture, incorrect way of sitting, standing or working? Is it a product of tension in our day-to-day life, a way to relieve frustration? Or is it due to some mechanical problem in the neck or head itself?In the 5th century, it was thought that a headache was due to a severe chill, exposure to sunlight, or even fatigue. In the 11th century, it was thought that it occurred after having cold things in our food. According to Tissort (1784), vomiting often concluded an attack. He also suggested that a reflex irritation of the gastric nerves resulted in an attack of migraine. Living (1873) said that a headache was related to asthma and a convulsive state. Rilay (1932) suggested that it occurred when noxious vapor entered the cerebral blood vessels. According to another opinion, it occurred due to eye strain. A few researchers concluded that it was due to adhesions of the cerebral membranes and formation of excessive cerebro-spinal fluid. Disorders of the ovaries and thyroid were also thought to cause migraines. Emotional problems were also attributed to headaches - for instance, a difficult father-and-son relationship in business, tough competition, a tense situation in the family, a hard struggle to get oneself established .... Apart from this, certain foods were found to cause headaches: chocolate, cheese, fruits, alcohol, fatty fried foods, tea, coffee, sea food, pork and many more.
RemediesThe long series of researches in this direction have shown that the human race has suffered a lot from headaches and though thousands of remedies have been prescribed, they have only succeeded in providing temporary relief Many migraine clinics and foundations have spent millions of rupees to find a remedy which will bring permanent relief These efforts are akin to ploughing in the sand! How long have we to live with such strong medications which produce side-effects in other systems of our body? After using a particular medicine for a long time, it loses its effectiveness anyway.
Sometimes, while suffering from a headache, a striking idea, solution or news gets rid of the headache and the patient becomes normal again. During a battle, General Ulysses S. Grant was seized with an attack of migraine. The limping general received the good news that his enemy was ready to surrender. Ulysses sprang to his feet at this glad news, and his headache vanished miraculously.
Many victims change their environment, take to the Himalayas, Tibet or Somaliland, go from the highest altitude to the lowest, from the wettest to the driest, experiencing a new climate, food and cultural changes but the migraine remains, because they carry their personal environment with them.
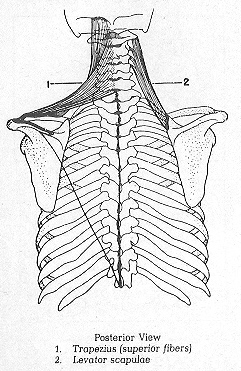
Headache of Cervical OriginFrequently, a chronic headache resistant to treatment is due to a disorder of the cervical spine, which may be cured by manipulation. Certain mechanical changes in the cervical spine may cause an intermittent or a continuous headache. These changes respond well to manipulation. The pain can spring from the neck. Some people do not believe in the possibility that pain can radiate from the neck to the head.
An experiment was carried out by Kellgreen. A concentrated saline solution was injected in the area where the cervical spine first joins with the head, producing tenderness and headache in the forehead region. This proved a connection between the neck and the forehead.
Important changes have been found in the cervical spine in cases of headaches. These relate to disturbances in the lumen of the vertebral artery which passes through the transverse process of the cervical vertebrae and supplies blood to the brain.
Sometimes the therapeutic effect of cervical manipulation helps us to confirm whether a particular headache is of cervical origin.
Sometimes a headache is produced by the head being kept in a certain position; keeping it in the opposite direction relieves the headache. Sometimes manual traction at the neck relieves the headache. These are indications that headaches may be of cervical origin, and manipulation succeeds.
Embryological, the head and the first and second cervical vertebrae are formed by the first and second cervical segment.
As they originate from the same segments they ought to have some relationship between them. So any abnormality at the level of the first and second cervical vertebrae can give rise to pain in any part of the head, the temple and the forehead. As it happens elsewhere, local pain at the level of the cervical vertebrae may be completely absent and the patient may complain only of a headache.
This type of headache may come on while waking up in the morning. It may be felt in the back of the head or the front of the head, or may be only in the forehead. This begins to ease after some hours and is much better by mid-day. The patient is free from headache till the next morning. As the years pass by, the headache may tend to last longer during the day. It responds well to manipulative treatment.
Dr Bicker's staff is of the opinion that headache is due to stretching or tension in the muscles, vessels or the outermost sheath of the spinal chord. If it is due to these mechanical reasons, the pain starts in the upper neck muscles, and spreads to the upper back and head. Instead of being limited in this area, it spreads to the entire head. It may be associated with stiffness and pain in the upper neck. It occurs off and on. The -headache seems to spread from the neck to the head rather than from the head to the neck.
There can be other causes of headaches too. Keeping that in mind, a detailed history of the patient can help in pinpointing the cause of the headache.
At times differentiation is difficult. But distinction is important, as headaches arising from the neck can most easily and lastingly be relieved'. So it is a great pity when the right diagnosis is not made and the right treatment is not administered. Am old man is often told that his headache is due to high blood pressure. In fact, it may be completely unconnected and it may be due to upper cervical osteoarthritis. Cervical manipulation can relieve pain on the lateral side of the face. This pain often has rhythmically and may be associated with a running nose or watering of the eyes. It may radiate to the upper jaw or even the lower jaw. The patient is often referred to a dental surgeon or oral surgeon.
Osteopathic examination may show tenderness over the side of the second and third cervical vertebra on the same side, and if the X-ray picture is clear, manipulation will be successful in many cases and the pain will subside.
Other Possible Causes of Headaches• Eye strain due to defective eyesight
• Sinusitis
• Toothache
• Digestive disturbances
• Neurological problems, e.g., an intra-cranial tumour
• Allergy
• Cardiovascular diseases
• Psychogenic (mental) frustration
Upper cervical pain may be caused by:
An intra-cranial tumour of the posterior fossa (portion) of the skull.
A disease of the upper cervical spine such as tuberculosis,
Malignancy
MigraineHeadaches occurring at intervals on the right or left side of the head, are associated with nausea and vomiting. There may be a feeling of seeing non-existent objects in front of the eyes before the onset of the headache. Such headaches usually start before the age of 30.
Many such patients respond to manipulation. In some cases Migraine may occur at the back of the head. In such cases manipulation will relieve the headache to a considerable degree.
Migraine of Cervical Origin. Spondylosis and osteo-arthritic changes in the cervical spine can cause an inflammatory reaction. This causes a spasm in the vertebral artery and its branches, resulting in a headache with the following characteristics:
1. It is mostly localized in the forehead and may be associated with nausea and severe vomiting. The headache always occurs on the same side. Manipulation elicits a good response.
2. Sometimes the headache is localized at the back of the eyeball and the initial symptoms pertain to visual abnormalities.
Case HistoriesA girl, eleven years old, had a severe headache for five days. She underwent laboratory tests of blood, urine, and stool. X-rays were also taken. Every finding was normal and the cause could not be detected. In spite of all possible medication she did not show any improvement. She was thought to be a case fit for a psychiatrist. But her father brought the child to me and narrated the following history: she complained of upper back pain when she went to school with a heavy bag strapped across her shoulders. This pain continued till late evening. She became irritable and would not listen to her parents.
The history of irritability and failure of drugs proved that her ailment was not physical but mental. She was treated manipulatively three times and her headache completely disappeared. She was taught to walk straight instead of going about with a forward stoop. She showed complete recovery.
A 29-year-old lady with three children had been getting headaches off and on since her college days. She also suffered from severe pain in the neck and both shoulders. The headache would occur twice or thrice a month during the day, lasting each time for 10-20 minutes. It would become less during the menstruation cycles. After she got married, the headaches went on increasing in frequency and intensity, and for two years she got headaches every day and had to resort to pain killers. The headaches were accompanied by tension in the neck and were more intense at the back of the head and in the frontal area, in her eyeballs and behind them.
Her condition was diagnosed as migraine. She was given manipulative treatment for her cervical spine and upper dorsal spine. Gradually the headaches started getting less frequent and less intense. She rarely used a pain killer. In 10 weeks the headaches completely subsided.
A 36-year-old engineer employed in the Railways had been suffering from headaches since his school days. They used to occur at fortnightly intervals and later, almost every week. The pain was very severe, starting from the back of the head and then spreading all over the head. He also felt pain in the upper back. His veins became prominent in the temples during the attack, and throbbed. He suffered from nausea and vomiting and would turn away from food or drink. All this would last for twenty-four hours, sometimes even for two to three days. Occasionally, when there was no severe headache, there would be a feeling of general uneasiness. He would prefer to remain in the dark and not be disturbed. He also preferred to lie down till recovery. He was given glasses as his sight was found to be weak, but this did not help. He consulted many doctors and took treatment, but to no avail.
He came to me with his complaint. I examined him thoroughly and found him to have a round upper back. X-rays of the cervical and dorsal spine were taken, but they did not reveal any abnormality; other pathological tests too were all normal.
Manipulative treatment was started. He felt no improvement after the first session. He was called again after a week and manipulative treatment of the cervical and dorsal spine was repeated. He felt some improvement. After a few weeks, his headache became less severe and less frequent. In three months he felt completely recovered, but he continued to come once a month for three months. He has since been advised to come twice a year for maintenance treatment. He has had no attacks ever since.
A young girl aged 21 years suffered from headaches for eight years. At first, she used to have a headache once a month or once a fortnight. During the last three years, the headaches became more frequent and she started having headaches almost every day. The ache was in the entire head, though more severe in the forehead. She did not get nausea or vomiting. Due to the severity of the headaches, she had to discontinue her studies. She was examined by a few doctors but nothing seemed to help her.
She was then referred to me for manipulative treatment. After being treated for three weeks, she felt much better. By the end of six weeks, she was completely cured and the headaches never returned. She has resumed her studies happily.
A good website for more information:
http://www.headaches.org/