Correctly Coding for OMT: Consistency Counts for OMT Coding
Summarized from this source: Consistency Counts for OMT Coding by Douglas J. Jorgensen, DO, CPC , ACOFP website.
Five Steps to Correctly Coding for OMT visits:
1. Perform and document a thorough history and examination.
2.Determine, perform and document theraputic and diagnostic intervention.
3. Put Somatic Dysfunction and the OMT Code first on encounter forms "Somatic Dysfunction as noted above" in your dictation.
4. List secondary diagnosis on encounter forms and in dictation.
5. Use the -25 Modifier on the E&M Code for your secondary diagnosis.
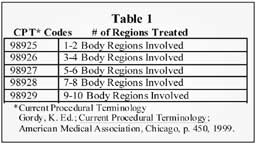
OMT codes are Current Procedural Terminology (CPT) codes designed to reimburse us for performing manipulative medicine on our patients. See Table 1 below for codes:
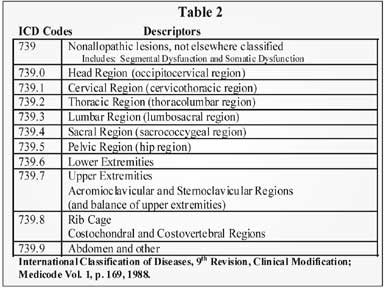
They are broken down by numbers of regions and are intended to correlate with the somatic dysfunctions ICD-9-CM codes regarding the specific regions treated. See table 2 below.
Documentation
When documenting OMT, use the documentation guidelines three key components of history, examination and medical decision making (MDM).
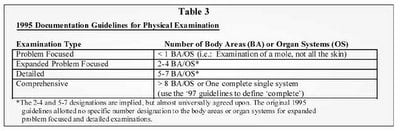
The history should have a chief complaint, history of present illness, review of systems and a past medical, family and/or social history. Your physical examination would include your musculoskeletal structural examination and any germane body area or organ systems. The history and physical examination should contain information germane to the complaint or be part of a workup to rule out specific pathology. One should not add components to the history or physical simply to enhance the documentation.
The MDM must evaluate the number of diagnoses, the amount of data to be reviewed and the level of risk involved depending on the type of problems found as well as medical and/or therapeutic intervention needed. Once the history, examination and MDM are scored an E&M code is assigned.
Evaluation &Management Codes
Consults come in two types: outpatient consults (99241-99245) and confirmatory consults (99271-99275). The first type (99241-99245) is used when another provider sends someone to be evaluated and treated. The confirmatory consult is for a new patient with a specific complaint, but you could use the outpatient codes for a new patient (99201-99205) also.Confirmatory consults are acceptable and are assigned a more optimal RVU designation than new patient codes. If you use the consult codes you must send a letter to the referring provider. A ‘cc’ or photocopy of your note is unacceptable unless you send a letter or fax stating you saw the patient and that your note is en route. This can be a form letter (see Figure 1), but even if the referring doctor is within your group practice, a written response from the consultant is still required. Lastly, dictating your office visit into letter format provides another option. 
25 Modifier
Modifiers are designed to better describe a code or how that code is being used in conjunction with another code or modifier. Typically it is used for two unrelated problems such as a treating a UTI at the time of an excisional biopsy.
With OMT, the diagnosis somatic dysfunction is listed first with the correlating ICD code(s) and CPT code without a modifier. The second, third and/or fourth diagnoses are listed and these justify or create medical necessity for the E&M service billed (your consult, in or outpatient codes). The E&M code gets a modifier here just like the UTI example, but the E&M code need not be for a separate problem and can in fact be what prompted the OMT.
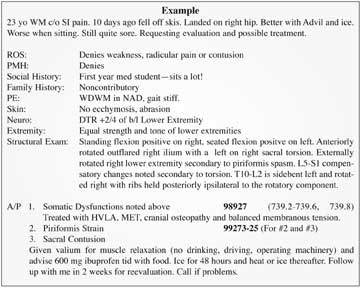
A Final Example:
0 Comments:
Post a Comment
<< Home